
Upcoming, highly-anticipated gene therapies for progressive muscle-degenerating disease Duchenne muscular dystrophy (DMD) will cost a whopping $2 million per patient per year—double the cost of the current standard-of-care, exon-skipping therapies—says GlobalData. The leading data and analytics company’s research highlighted the costs of various DMD treatment types as part of an assessment of the upcoming pipeline, as well as investigated to what extent the pipeline will meet the needs of DMD patients.
Chris Pilis, Immunology Analyst at GlobalData, comments: “Aside from the highly genericized prednisone, therapies targeting DMD are very expensive. Exon-skipping products cost around $1 million per patient annually (depending on weight) and Emflaza, a second-generation steroid agent, costs approximately $175,000–275,000 per year.*
“The much-anticipated gene therapies that are currently in Phase III—namely Pfizer’s PF-06939926 (fordadistrogene movaparvovec, NCT04281485) and Sarepta Therapeutics’ SRP-9001 (delandistrogene moxeparvovec, NCT05096221)—are estimated to cost around $2 million per patient annually, while other candidates’ prices will have an annual cost between that of Emflaza (deflazacort) and exon-skipping products.”
The DMD treatment market has great unmet need, as patients currently have limited treatment options with relatively poor safety and efficacy profiles. GlobalData highlights some of the key needs to include therapies that delay or reverse disease progression; improved options for patients that are not able to walk due to DMD; and reductions to the high cost of therapy.
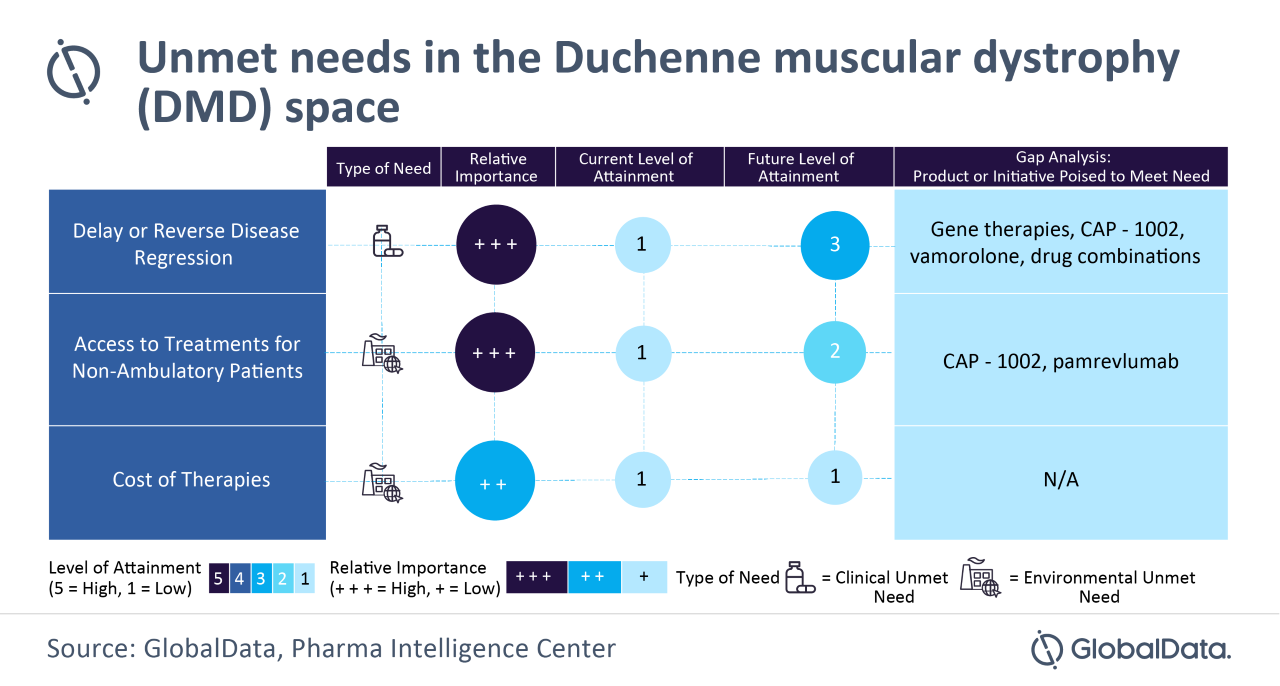
Pilis continues: “GlobalData expects that the pipeline drugs will only partially address the needs of DMD patients. While they are expected to have better efficacy and tolerability profiles, non-ambulatory patients are still expected to have limited treatment options and the cost of therapy is not anticipated to reduce due to the rarity of the disease.”
What are the key pipeline therapies?**
- Translarna (US & Japan), Expected to be available by 2022 – A small molecule that interacts with the ribosome to enable it to read through premature nonsense stop signals on mRNA and allow the cell to produce a full-length, functional protein.
- Movap. (Pfizer) (US & Japan), 2025 – In vivo gene therapy that uses a recombinant adeno-associated virus serotype 9 (rAAV9) capsid to deliver a shortened version of human dystrophin gene to produce a shorter than normal dystrophin, called mini-dystrophin.
- Mox. (Sarepta) (US), 2025 – In vivo gene therapy intended to deliver the micro-dystrophin-encoding gene to muscle tissue by utilizing an AAVrh74 vector for the targeted production of the micro-dystrophin protein.
- Givinostat (US), 2022 – Anti-fibrotic small molecule that inhibits histone deacetylases, enzymes involved in turning genes on and off within cells. It also inhibits several pro-inflammatory cytokines. It can be used regardless of the dystrophin gene mutation type.
- Pamrevlumab (US), 2024 – Monoclonal antibody that inhibits the activity of connective tissue growth factor (CTGF), a critical mediator in the fibrosic process that is developed in DMD. It can be used regardless of the dystrophin gene mutation type.
- CAP-1002 (US), 2024 – Cell therapy developed by Capricor that claims to modify the immune system to encourage cellular regeneration of mainly cardiac and potentially skeletal muscle cells – it is planned to be administered every three months for a single year. It will mostly be administered to late ambulatory and non-ambulatory patients as it mainly targets the myocardium).
- Vamorolone (US), 2022 – Synthetic steroid that claims to have a similar efficacy profile to current steroid treatments, but with fewer side effects (in comparison to clinical trials with other steroids, long-term treatment with vamorolone resulted in fewer side effects than typically observed for example with classic steroid prednisone).
- Pizuglanstat (Japan), 2027 – A selective hematopoietic prostaglandin D synthase (HPGDS) inhibitor that aims to reduce inflammation caused during muscle damage in DMD. It can be used regardless of the dystrophin gene mutation type.
GlobalData offers its view on the pipeline and opportunities available:
Chris Pilis comments: “Currently, patients that are no longer able to walk (ambulatory) need to discontinue exon-skipping therapy for patients with amenable mutations, leaving steroids as the only treatment option. The lack of treatment options for these patients creates an opportunity for pipeline agents such as FibroGen’s pamrevlumab and CAP-1002.
“If approved, these products could be useful as monotherapies or add-on therapies that can help reduce steroid dosage, and thus also reduce side effects. However, with the exception of pamrevlumab and CAP-1002, which are being studied in both ambulatory and non-ambulatory patients, most pipeline candidates are expected to initially be administered only to ambulatory patients until long-term safety data is acquired.
“There is still ample space for novel products to enter the market either as monotherapies or add-on therapies that can be administered in various combinations according to each patient’s needs.”
* Figures depend on weight: $175 million is the ACOT for the average pediatric DMD patient while $275 million is the ACOT for the average adult DMD patient.
** For the US and Japan market
